
Structural Biochemistry/Anthrax
History
[edit | edit source]The name Etymology comes from anthrax, which is a Greek word meaning coal. It derived from the Greek word meaning coal because of the black skin lesions developed by victims with a cutaneous anthrax infection. In the year 1875, a German physician named Robert Koch first identified the bacterium that caused the anthrax disease. His research was the first to show how microbes can cause disease. Koch uncovered the life cycle and reasons of transmission of anthrax. His experiments also helped understand the role of microbes in making people sick during the period when debates still took place over spontaneous generation versus cell theory. After discovering that bacteria caused tuberculosis, Koch won the Nobel Prize in Physiology or Medicine in the year 1905.
Furthermore, in May 1881 Louis Pasteur performed a public experiment to show his thoughts on vaccination. To demonstrate this, he prepared two groups of 25 sheep, several cows, and one goat. The animals of different groups where injected with either anthrax vaccine or left unvaccinated. IN the end it was found that all the animals in the non-vaccinated group died, while all the animals in the vaccinated group survived. Then in the year 1954, the human vaccine for anthrax became available and in 1970 the improved cell-free vaccine was also made available.
Introduction
[edit | edit source]
Anthrax is a binary toxin that is secreted by Bacillus anthracis, which secretes the three proteins that composes the anthrax toxin. The anthrax toxin is composed of three proteins that are nontoxic alone, but creates a toxic complex together. The three proteins are Lethal Factor (LF), Edema Factor (EF), and Protective Antigen (PA). Lethal Factor and Edema Factor are enzymes and Protective Antigen is a multifunctional protein.
Structure
[edit | edit source]Native Protective Antigen (Native PA) is a long, flat protein that is composed of four folding domains. The first domain (Domain 1) is a β-sandwich with four helices and two calcium ions. The second domain (Domain 2) is composed of a β-barrel core and forms a pore that allows the Lethal Factor and Edema Factor into the cytosol. The third domain (Domain 3) has a ferredoxin similar fold. And the fourth domain (Domain 4) is composed of a β-sandwich with an immunoglobulin similar fold that is used to bind to cellular receptors, the fourth domain has minimal contact with the other parts of the protein.
-
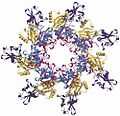 Heptameric Prepore structure.
Heptameric Prepore structure.

The Heptameric Protective Antigen Prepore is a ring with an empty interior and a flat hydrophobic surface, which is the binding site for the Lethal Factor and Edema Factor. It has a mushroom shape.
-
 Lethal Factor structure.
Lethal Factor structure.

The Edema Factor has a pocket that binds to the host cell and causes the cell to fill with fluid. The edema factor is nontoxic alone, but changes shape upon binding. The active site of the Edema Factor enzyme is a promising drug target because the pocket can be easily blocked. The lethal factor is a Zn2+ dependent endoprotease.
ANTXR1 and ANTXR2 are two cell receptors that bind PA. ANTXR1 is a medium length receptor and ANTXR2 is a long receptor. These two receptors are present everywhere on extracellular domains.
Mechanism of Toxin
[edit | edit source]
The anthrax toxin starts working when the Protective Antigen (PA) binds to either of the cellular receptors ANTXR1 or ANTXR2 and becomes proteolytically activated. Then, the Protective Antigen forms the Heptameric Prepore (PA oligomerizes to form the hollow ring). This new prepore binds to either or both of the enzymatic components of the toxin: Lethal Factor (LF) or Edema Factor (EF). The complexes made upon the binding of these enzymes is moved to the endosome; the prepore turns into a transmembrane pore and the Lethal Factor and Edema Factor cross through the pore to the cell cytosol.
Once inside the cell, Lethal Factor cuts and disables protein kinases (MAPKK 1 and MAPKK 2) that are involved in the activation of proteins vital to the cell. The Edema Factor inhibits immunological response and causes cell death.
Anthrax in Humans
[edit | edit source]Although anthrax is an infectious disease that typically affects animals, humans who come into contact with animals infected with anthrax can become infected as well. When humans have the infectious disease, the infection usually involves the skin, gastrointestinal tract, or lungs.
Routes of Anthrax Infection
[edit | edit source]With cutaneous anthrax, the most common type of anthrax infection, it usually occurs when an anthrax spore comes into contact with a cut or scrape on a person's skin.
Inhalation anthrax develops when a spore enters the lungs. Breathing in an anthrax spore does not indicate that a person will be infected with anthrax disease. It indicates that they have been exposed to anthrax. For inhalation anthrax to fully develop, the bacterial spore must sprout in order for the actual disease to take place. This typically takes 1 to 6 days. If a spore sprouts, it releases toxic substances wich can cause internal bleeding, swelling and tissue death.
Gastrointestinal anthrax occurs when someone consumes meat that has been infected with anthrax.
Symptoms
[edit | edit source]Cutaneous anthrax symptoms being to show 1 to 7 days after exposure:
- An itchy sore, similar to an insect bite, appears. The sore may blister and become black.
- Painless sore, but swells.
- A scab forms, and dries and falls off in approximately two weeks.
Inhalational anthrax symptoms:
- Fever, discomfort, headache, cough, shortness of breath (SOB), and chest pain
Gastrointestinal anthrax symptoms occur within a week and may include:
- Abdominal pain
- Normal or bloody diarrhea
- Fever
- Mouth sores
- Nausea and vomiting
Treatment
[edit | edit source]Anthrax infections are typically treated with antibiotics.
Those with inhalational anthrax are given a combination of antibiotics. Doctors usually first give the patient ciprofloxacin plus another drug, intravenously. Inhalational anthrax treatment typically takes about 60 days because spores can take up to that amount of time to sprout.
Cutaneous anthrax is treated through oral antibiotics such as doxycycline and ciproflaxin for about 7 to 10 days.
References
[edit | edit source]Croston, Glenn. "Anthrax Toxin Mechanism of Action ." Biocarta. N.p., n.d. Web. 30 Nov. 2011. <www.biocarta.com/pathfiles/h_anthraxPathway.asp>.
Karin, Michael, and Jin Mo Park, PhD. "Molecular Mechanism Underlying Anthrax Infection Described." UC San Diego Health System | San Diego Hospital, Healthcare . UCSD, 29 Sept. 2002. Web. 30 Nov. 2011. <http://health.ucsd.edu/news/2002/08_29_Karin.html>.
Young, John A. T.,Collier, R. John . "Anthrax toxin: Receptor binding, internalization, pore formation, and translocation." Annual Review of Biochemistry. Web. 30 Nov. 2011. <http://www.annualreviews.org/doi/pdf/10.1146/annurev.biochem.75.103004.142728>.
Images from Wikimedia Commons.